Augmentation of breast is done by using silicone implants under the breast gland, under the major thoracic muscle or under muscle or partially under muscle and under breast gland: dual plane positioning. In any case we prefer to operate under general anaesthesia after a complete evaluation of the patient’s measurements in the area of breast and thorax and also an evaluation of her somatotype to enable us to choose the best implant style and position and achieve an optimum aesthetic and functional result.
Theoretically there are three possible sites/incisions for the insertion of the implant: in the axilla , periareolar and in a natural fold under the breast which is preferable for many reasons: the breast is intact, the incision is hidden in a natural fold and therefore invisible in standing position.
This is the simplest and quickest method of permanent breast augmentation. Alternatively we can fat graft the breast using canuas after liposuction from all parts of the body –liposculpture, fat transfer – with or without external expansion of the breast – Brava System – but it is a time-consuming, repeated procedure (part of the fat is absorbed), suitable for mild breast augmentation.
AUGMENTATION WITH SILICONE IMPLANT
Before
1 month later
Immediately after pregnancy : normal breastfeeding
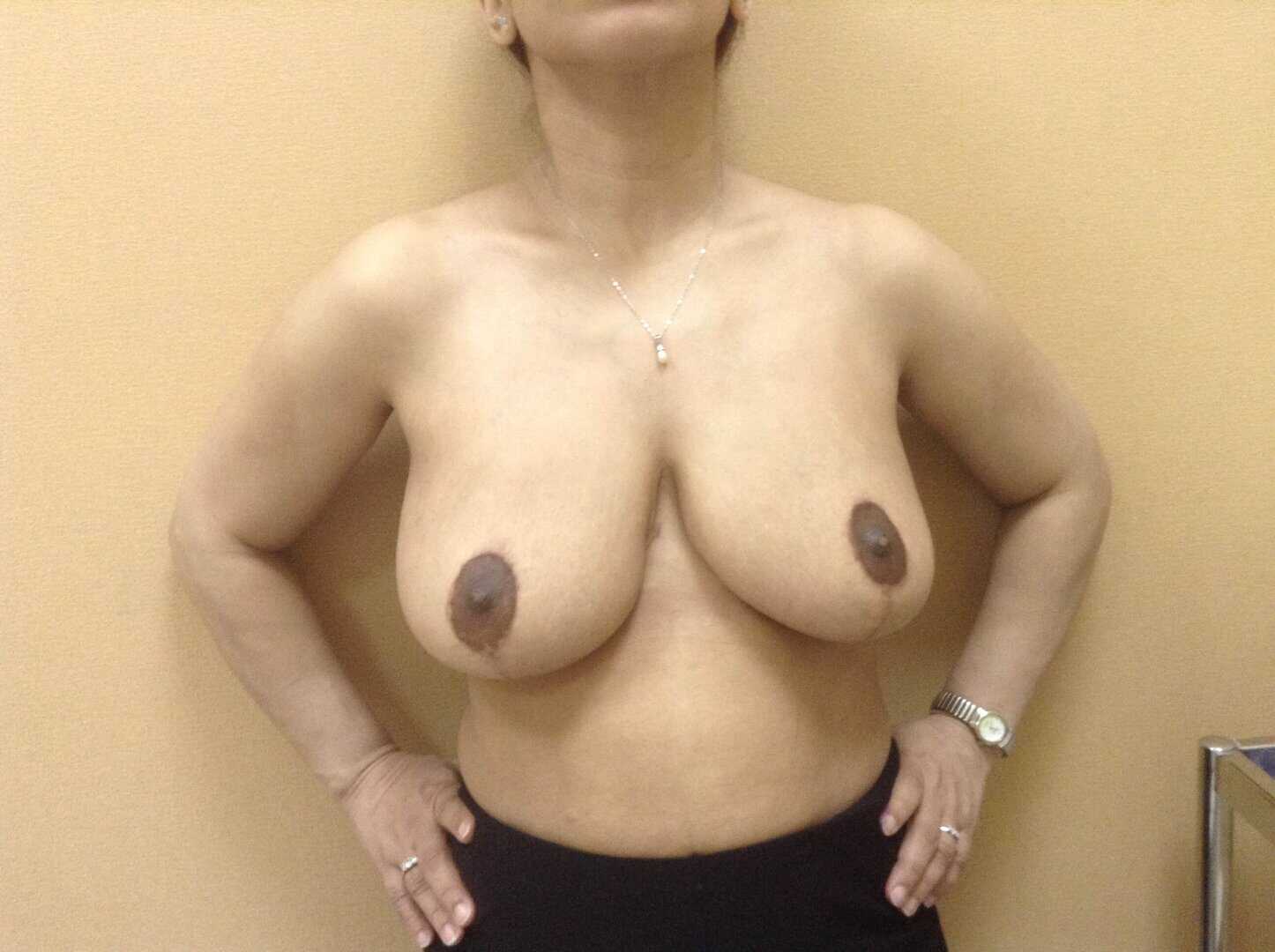
BREAST PTOSIS CORRECTION
It is one of the most popular, together with breast reduction, operations where we reposition the nipple areolar flap upwards and do remodeling and lifting of the breast from inside. External incisions are periareolar, with or without mid-vertical («L» shaped or inverted «T» shaped incision) depending on the width of breast and degree of ptosis and skin laxity.
The excess skin is removed and the breast is stabilized with internal sutures as well as external suturing of the skin pocket, that covers the breast and the fat tissue.
Before
After
BREAST REDUCTION
We follow a similar technique as in breast lifting but we also remove parts of the breast and fat from the base and lower lateral quadrants, especially the lower out quadrant, together with skin removal, after lifting and internal remodeling and supporting of the already ptotic and big breast.
BREAST ASYMMETRY - TUBERUS BREASTS CORRECTION
We follow a similar technique as in breast lifting but we also remove parts of the breast and fat from the base and lower lateral quadrants, especially the lower out quadrant, together with skin removal, after lifting and internal remodeling and supporting of the already ptotic and big breast.
BREAST RECONSTRUCTION POST MASTECTOMY
It represents the biggest challenge in breast aesthetics because except from the reconstruction itself we have to achieve symmetry to the other side of the healthy breast –lateral mastectomy.
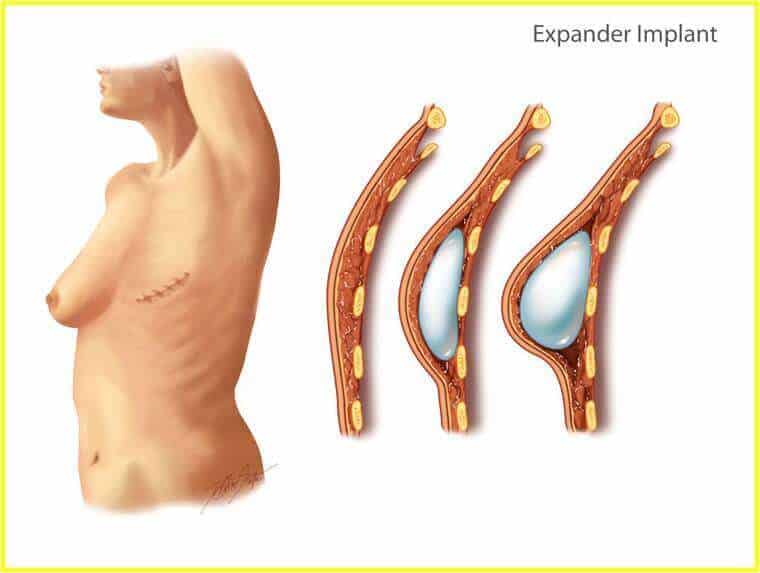
As per reconstruction, nowadays we strongly recommend immediate reconstruction ( at the same time with the initial mastectomy) at least with an insertion of a tissue expander under the muscle on the operated side – step one reconstruction.
Immediate reconstruction does not only have no oncological contraindication but it also provides a better aesthetic outcome, psychologically supports the patient and makes the reconstruction procedure faster compared with the late reconstruction (one operation less).
6 months after step one and after full expansion of the expander we proceed to its replacement with a permanent silicone implant in equal size and shape with the healthy breast – step two reconstruction.
Expander Restoration - Permanent Silicone Implant
During the 6 months before step two the patient completes chemotherapy and/or radiotherapy, if needed, depending on the breast cancer stage.
Step three – Final reconstruction takes place 6 months after step two. Under local anaesthesia and using multiple techniques we create a nipple and areola similar and symmetric to the healthy breast.
During this second 6-month period we can operate on the healthy breast, if needed, to reduce or lift it in order to achieve complete symmetry of the two breasts.
Latisimous Dorsi - Flap Reconstruction
Operation on the healthy breast, if needed, can also be done at the same surgical time with step two of reconstruction, (insertion of silicone implant on the operated breast).
We can also reconstruct the breast using autologous tissue of skin and muscule flaps: latissimus dorsi and rectus abdominis –tram flap or free flaps as free tram or gluteus muscle flap with each technique having advantages and disadvantages .
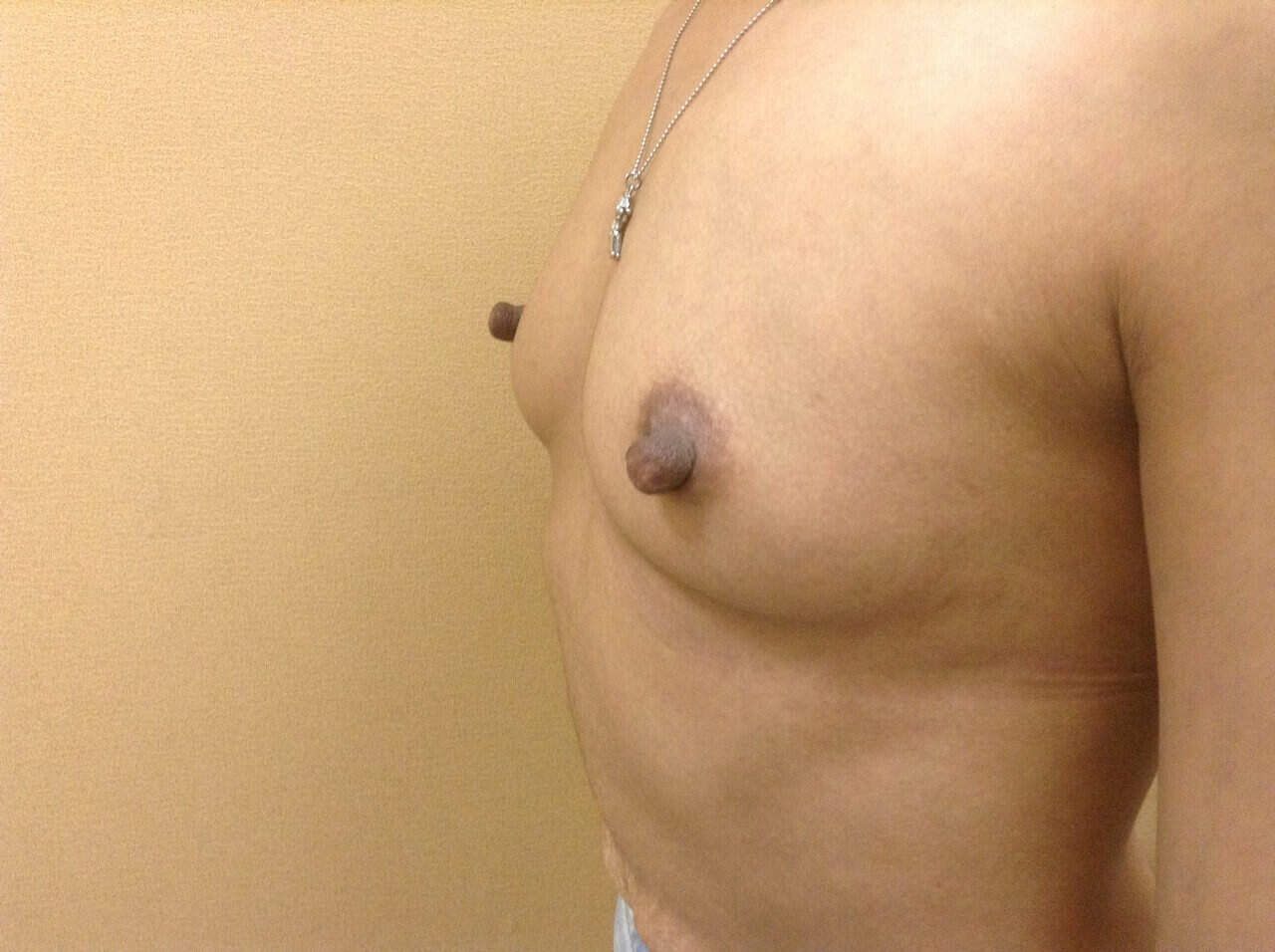
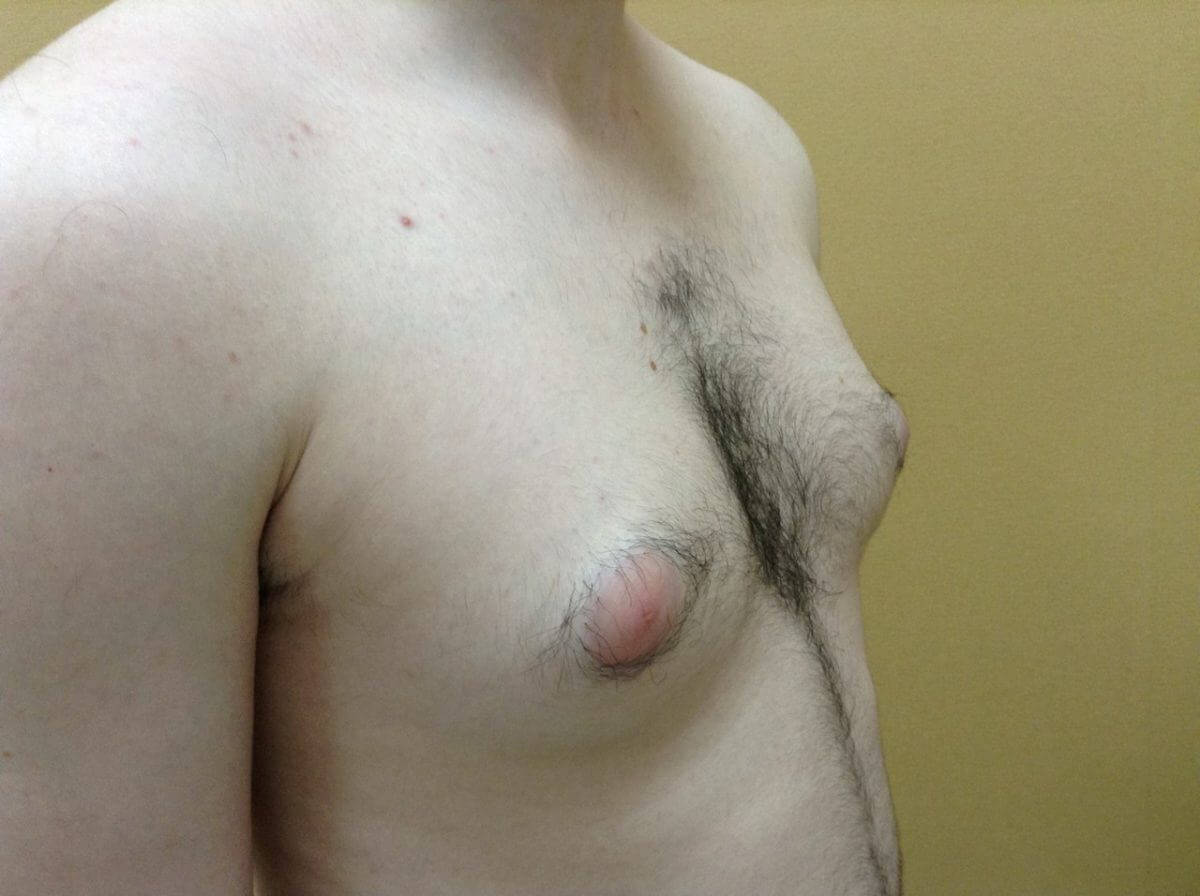
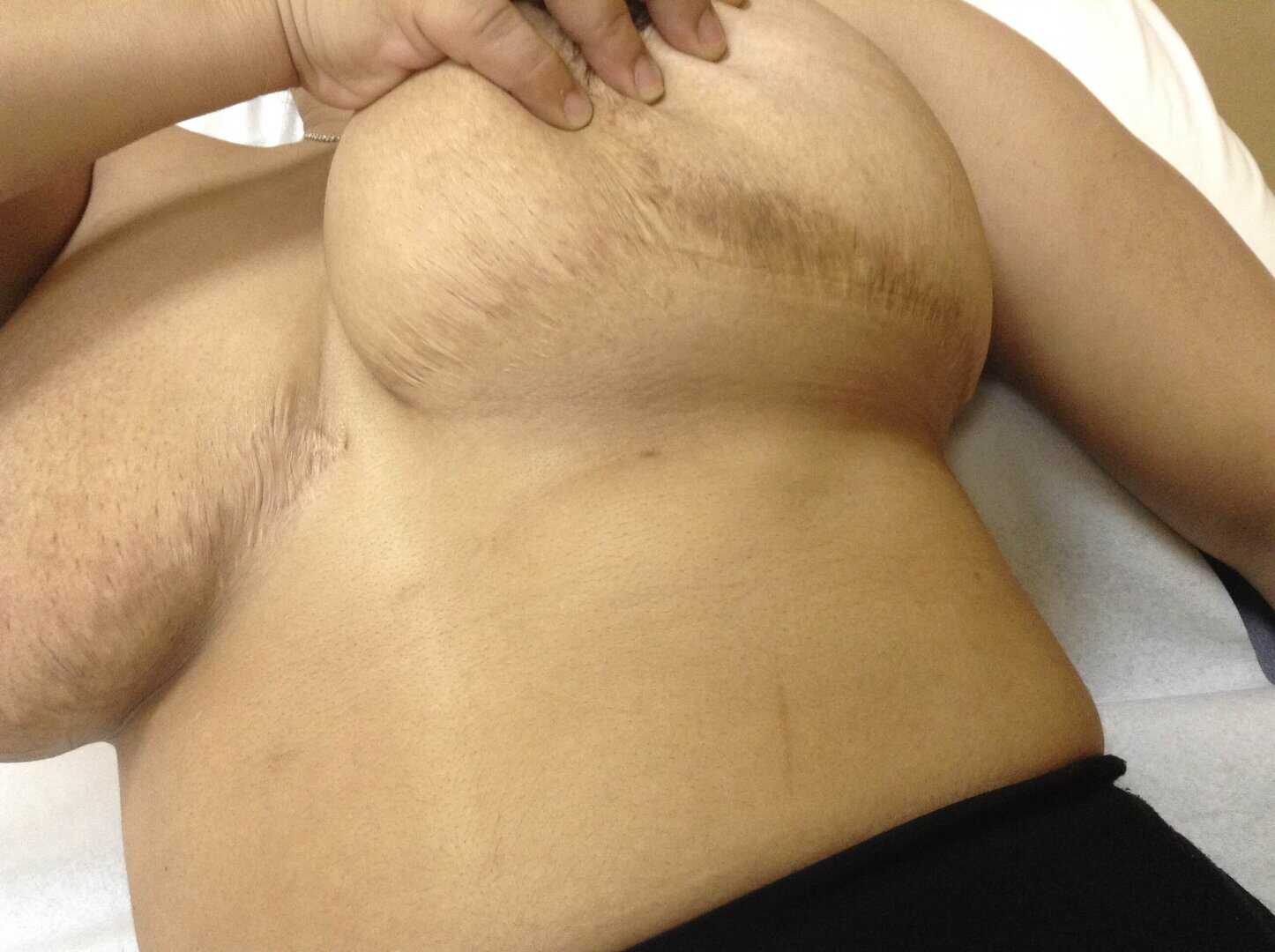
GYNAECOMASTIA CORRECTION
It is fair to distinguishh between true or false gynaecomastia. In the true one, we have actual enlargement of the breast gland while in the false one just excess fat. In any case the terminology is incorrect.
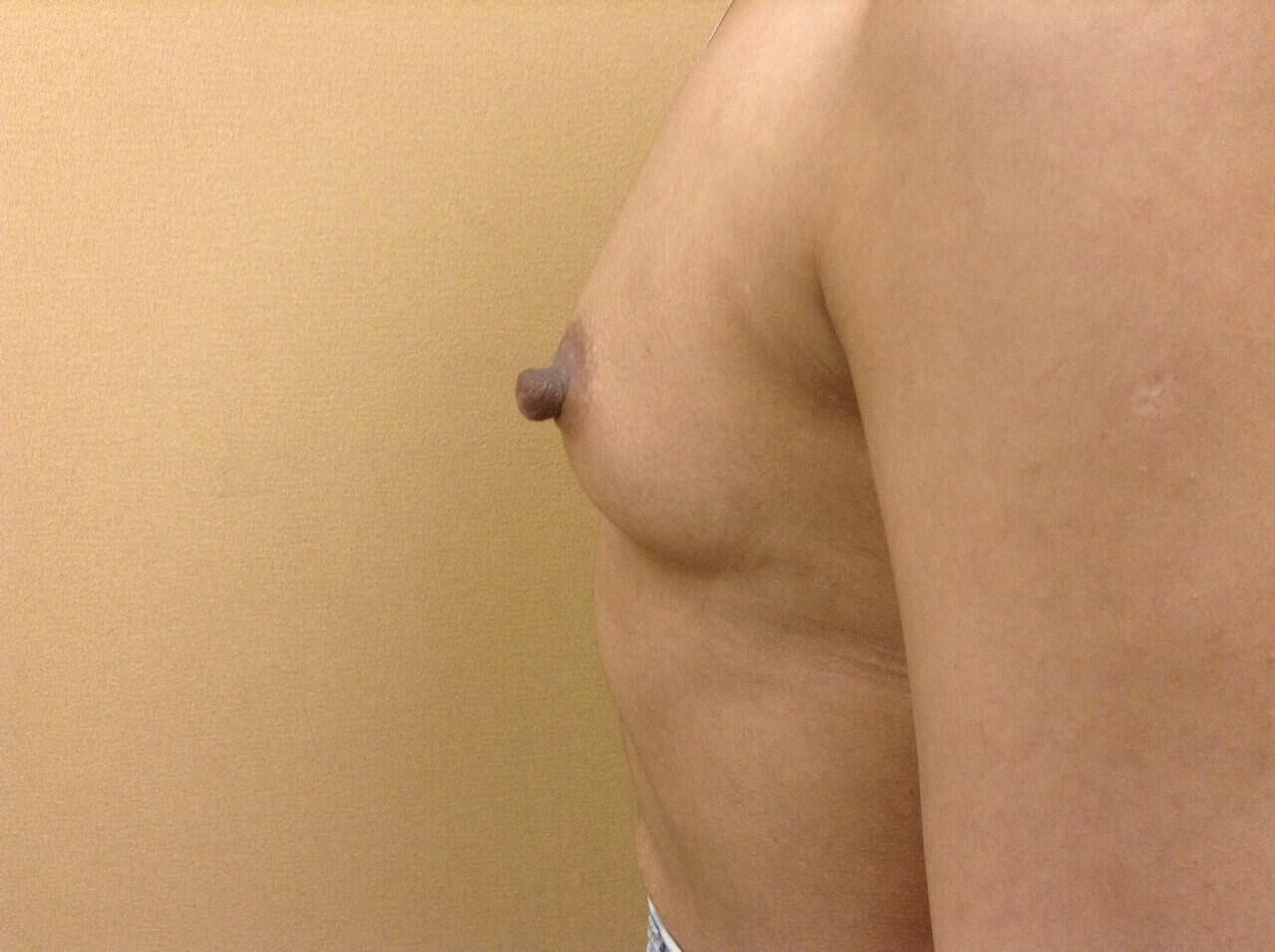
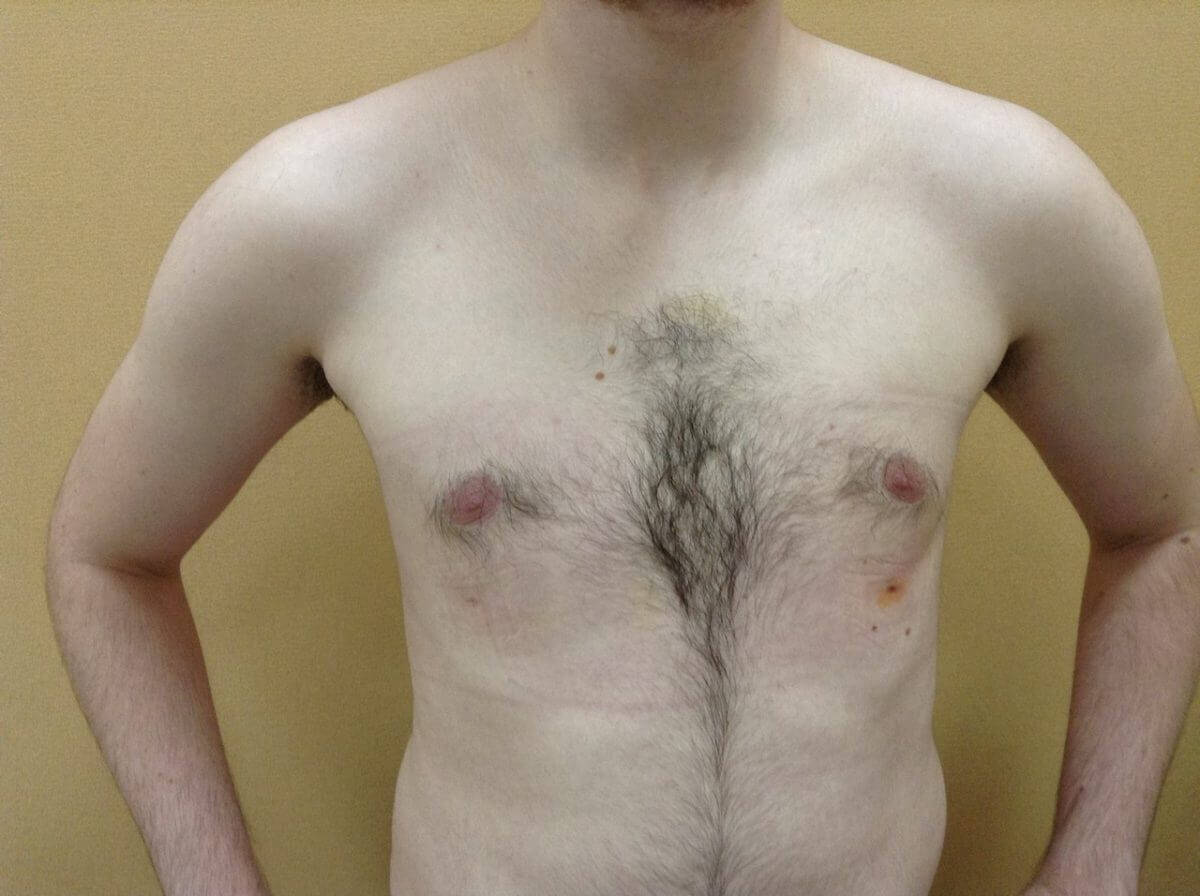
Depending on the case, we execute either liposuction or subcutaneous mastectomy ( just from a periareolar incision because scars are obvious on the thoracic wall of men) or a combination of these two methods.
MASTOPLASTY IN MAN
BEFORE
IMMEDIATELY AFTER
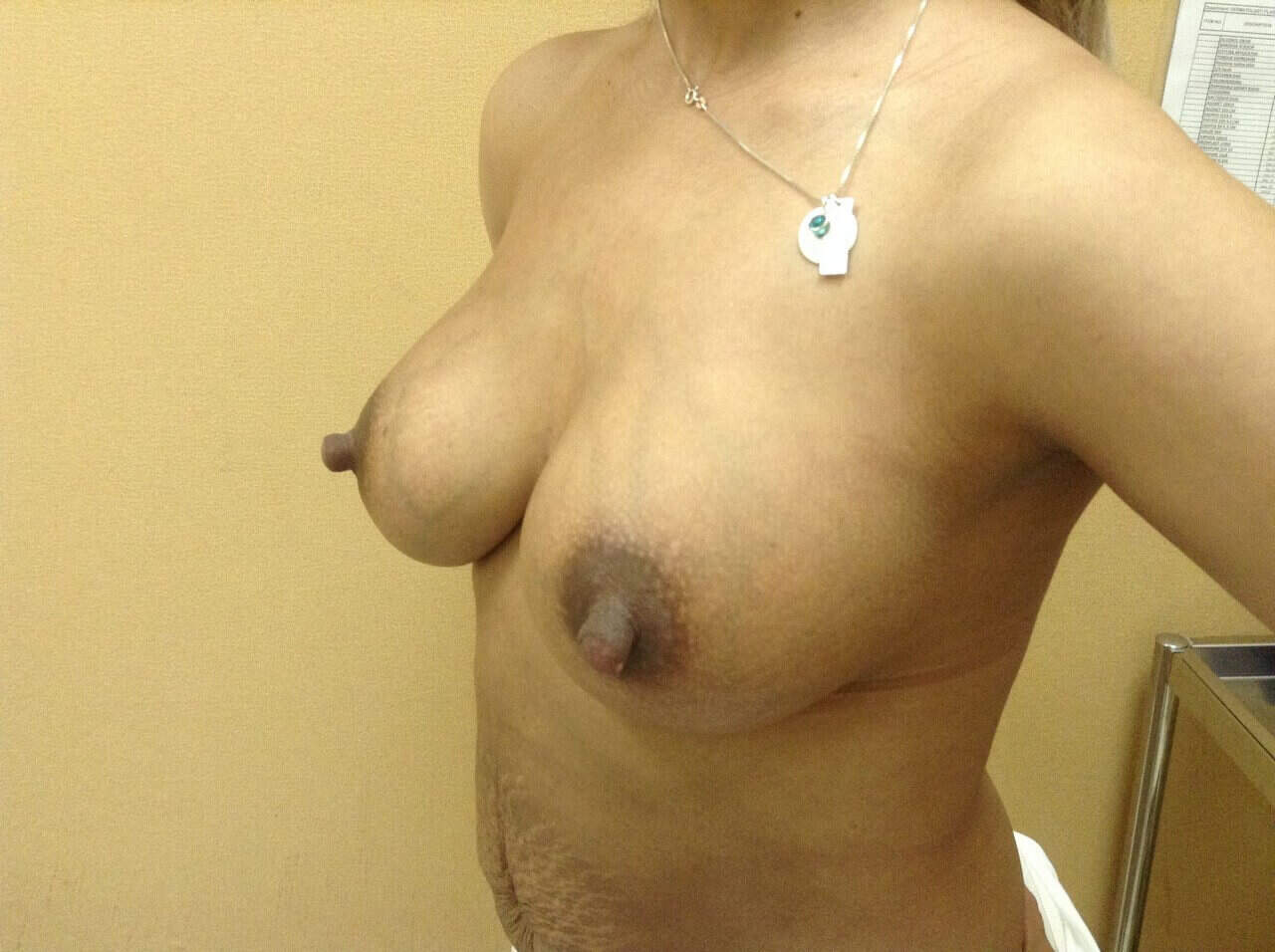
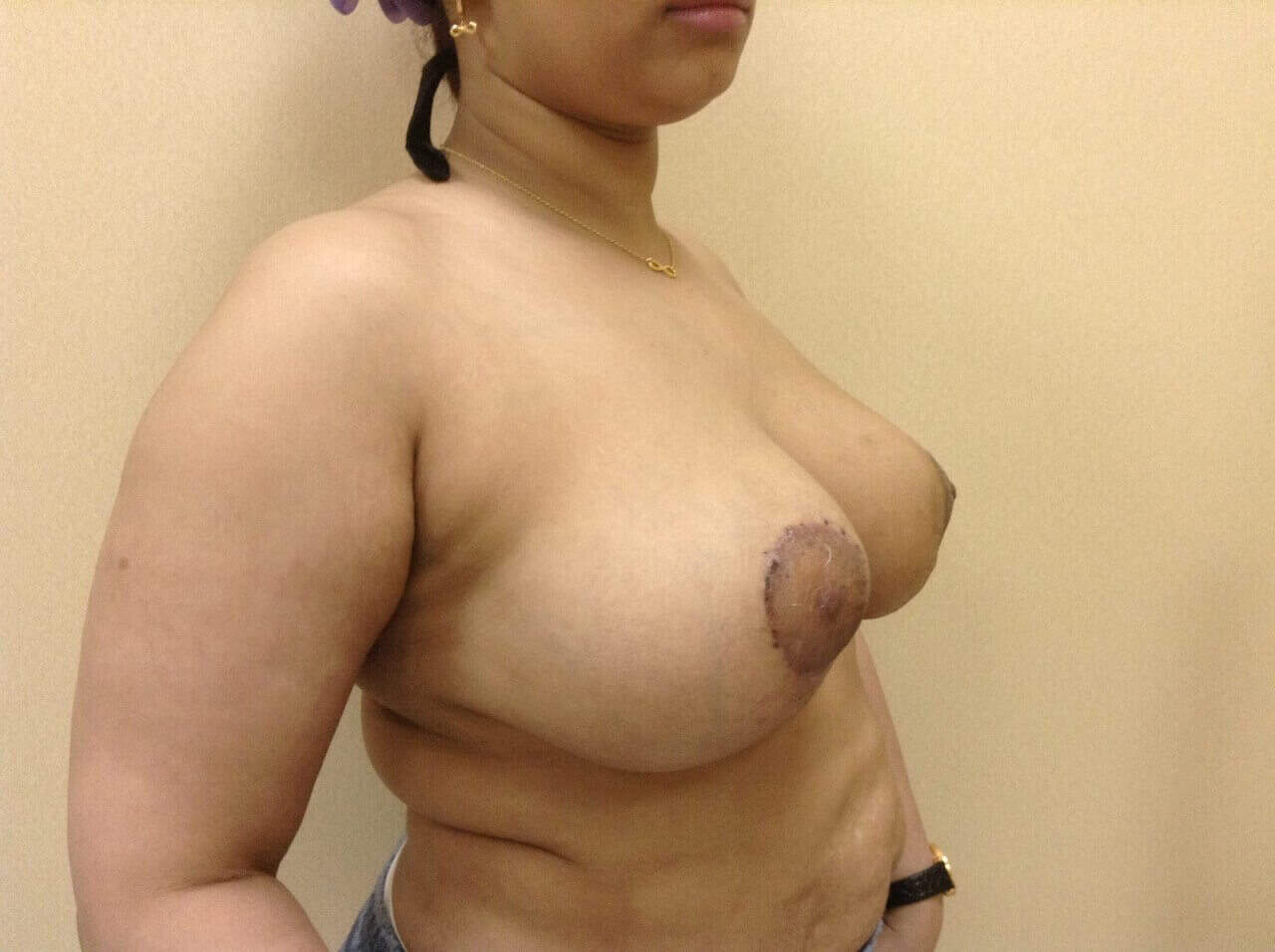
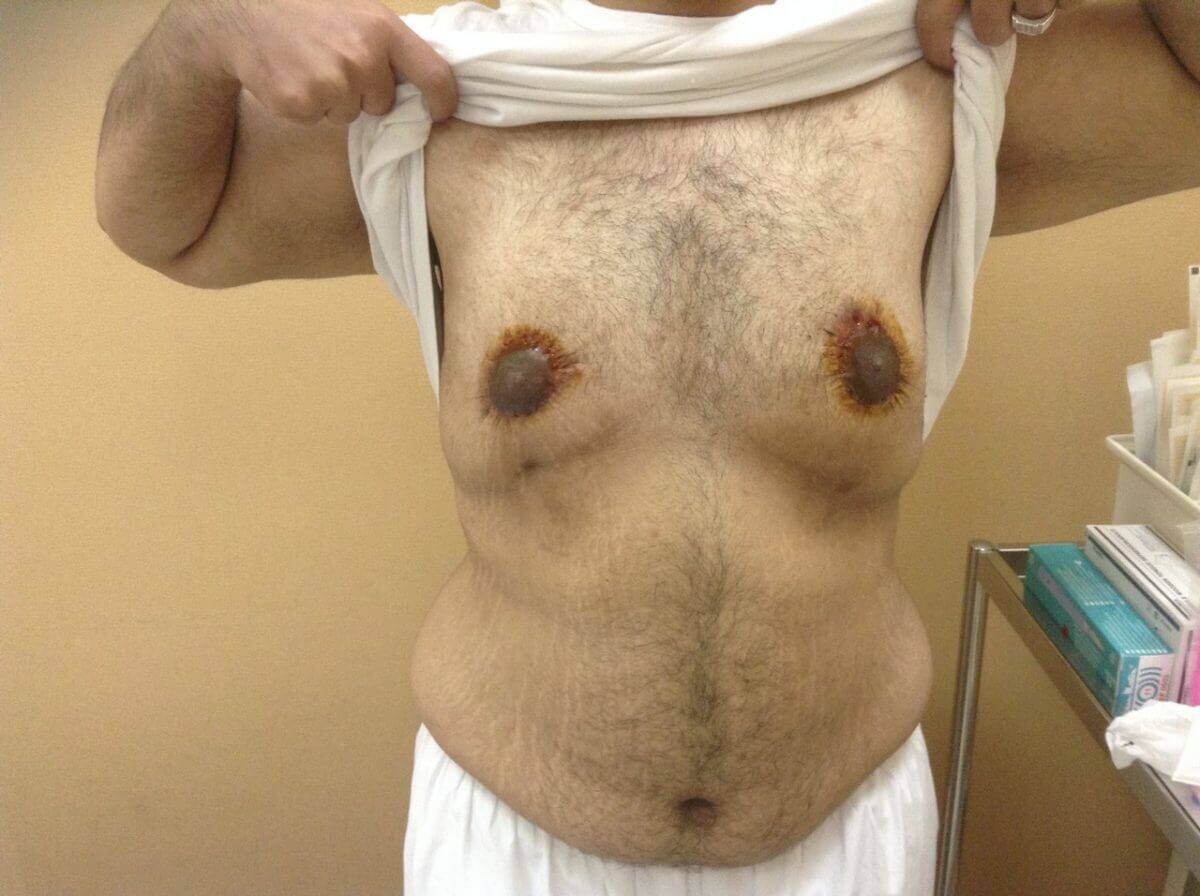
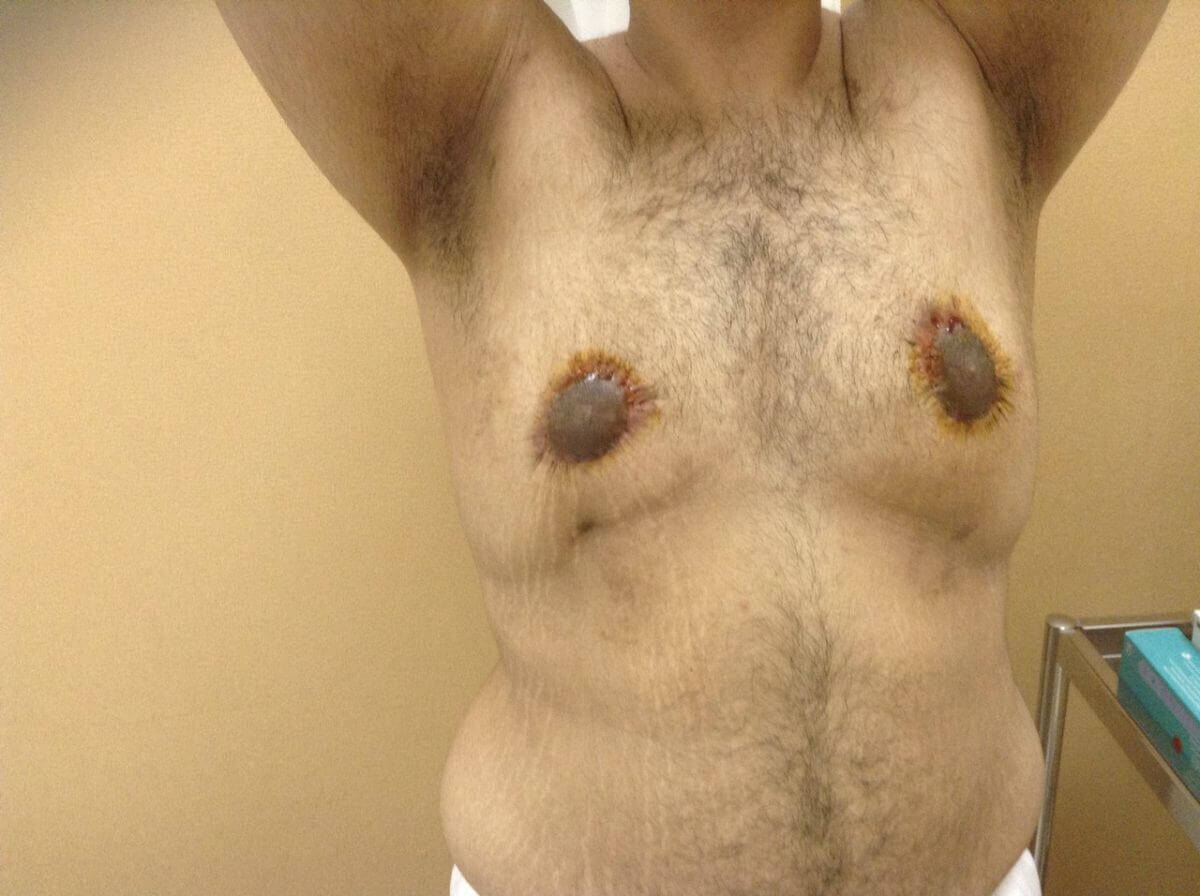
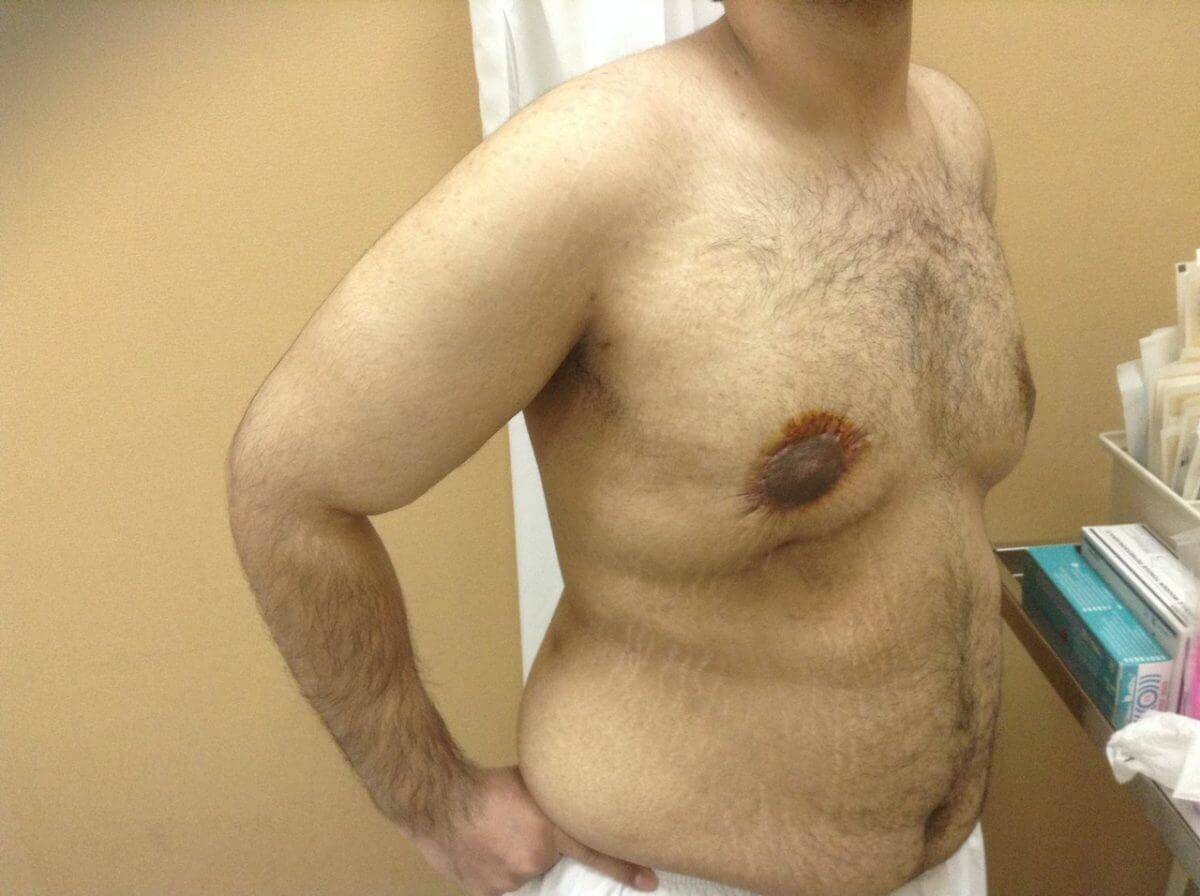
CIRCUMFERENTIAL PERIAREOLAR MASTOPLASTY
BEFORE
IMMEDIATELY AFTER
BARIATRIC PLASTIC SURGERY(BRANCHIOPLASTY, LIFT OF LEGS AND TRUNK)
This is a series of operations – except from abdominoplasty and mastoplasty – that refer to other body areas in the trunck and limbs where we correct laxity and excess skin after massive weight loss, and a year after the patient has stabilized his/her weight.
The incisions on the arms and legs can be either horizontal in the physical folds (in axilla and inguinal fold) or vertical in the inner sides of the arm or leg respectively in the upper or lower limbs.
On the trunk, incisions are created horizontally on the upper end of the gluteous area until they join the abdominoplasty incision- full trunk lift.
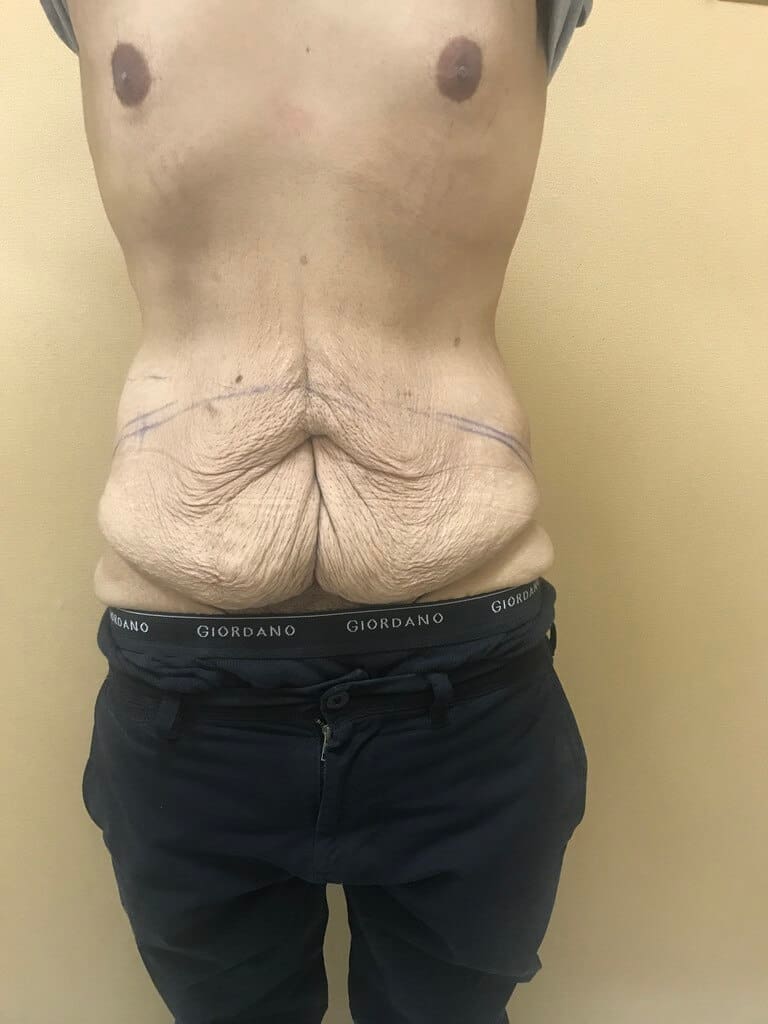
CORRECTION OF BREAST & ABDOMEN POST BARIATRIC
Before
After
CIRCUMFERENTIAL CORRECTION OF TRUNK LAXITY POST BARIATRIC
BEFORE
IMMEDIATELY AFTER
LIFT OF BREAST AND ARMS
Before
After
WET LIPOSUCTION, LIPOSCULPTURE
Liposuction is one of the most common interventions but it is not a way to lose weight!
It is the only and permanent way to correct local lipodystrophy of abdomen buttocks, knees and we prefer not to remove more than 5 liters of fat in total during an operation to maintain the electrolyte stability of the body.
There are different types of liposuction.
Wet liposuction is infiltration of the fatty area with local anasthetic and vasoconstrictive solution of normal saline -Tumescent Solution-equal volume to the amount of fat we wish to remove. The removed fat after special treatment can be grafted, with injections, in areas of the body that have lack of fat to achieve augmentation or symmetry –breast, buttocks and face.
This is called liposculpture of face and body or fat remodeling with liposuction and fat transfer – fat grafting -to obtain symmetry and harmonic appearance of body and face.
FAT TRANSFER
BEFORE
IMMEDIATELY AFTER
LIPOSUCTION OF LOWER ABDOMEN AND BACK
BEFORE
IMMEDIATELY AFTER
A YEAR AFTER
LIPOSUCTION OF LEGS
BEFORE
IMMEDIATELY AFTER
VESER LIPOSUCTION
It is a technique of liquefied fat suction, much less traumatic and almost bloodless. In the beginning we use a veser ultrasonic machine inside the fat tissue to liquify it and then, through the same holes, we suction the area with small cannulas.
It is preferable to wet liposuction because it is less traumatic, so less edema, bruising, pain and a shorter rehabilitation time.
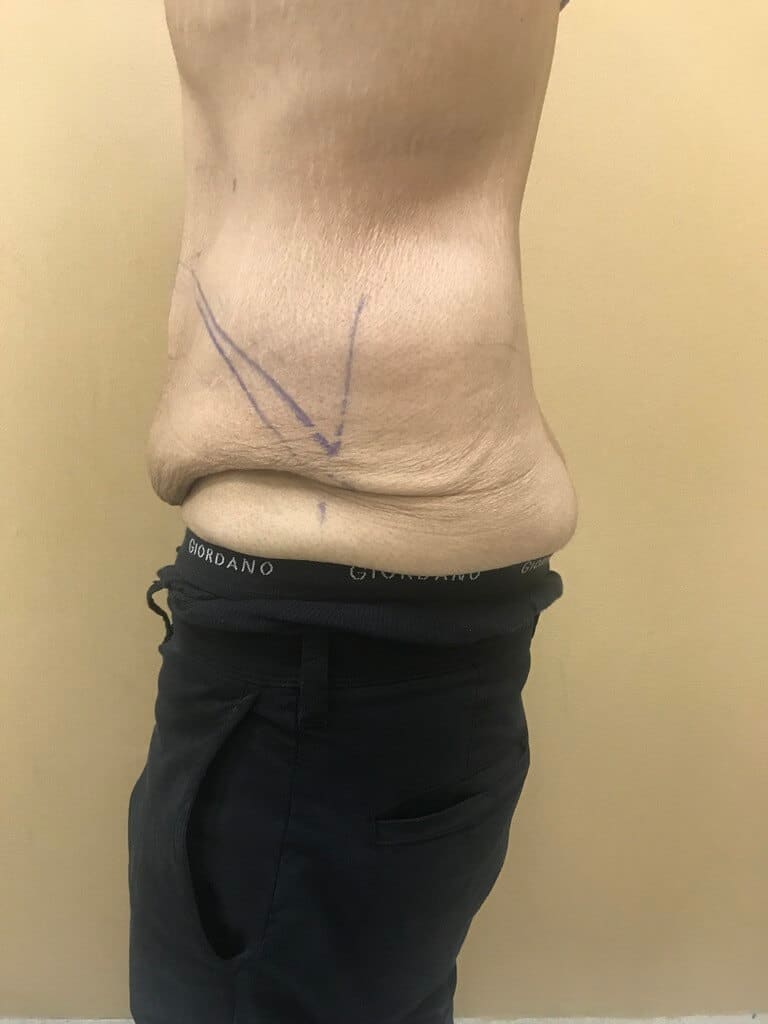
ABDOMINOPLASY WITH OR WITHOUT LIPOSUCION
It is a technique of reconstruction of abdominal wall laxity after big loss of weight or repeated pregnancies, and can be combined with liposuction if needed.
It is dermolipectomy of the excess lax skin and fat of the lower abdominal wall beyond the umbilicus (hanging abdomen) undermining and pulling down of the upper abdomen flap (over the umbilicus) and direct suture to the skin on the pubic area – cesarian incision site.
Before that we plicate the anterior rectus abdominis sheath to correct muscular laxity and support the abdominal wall and inner organs of the abdomen. This way we achieve a flat belly. We remove and stabilize the umbilicus flap to its new up position through a hall on the upper abdominal skin flap.
In all cases the operation is done under general anaesthesia and has a prolonged rehabilitation time, approximately 10 days.
ABDOMINOPLASTY WITH ABDOMEN LIPOSUCTION
BEFORE
IMMEDIATELY AFTER
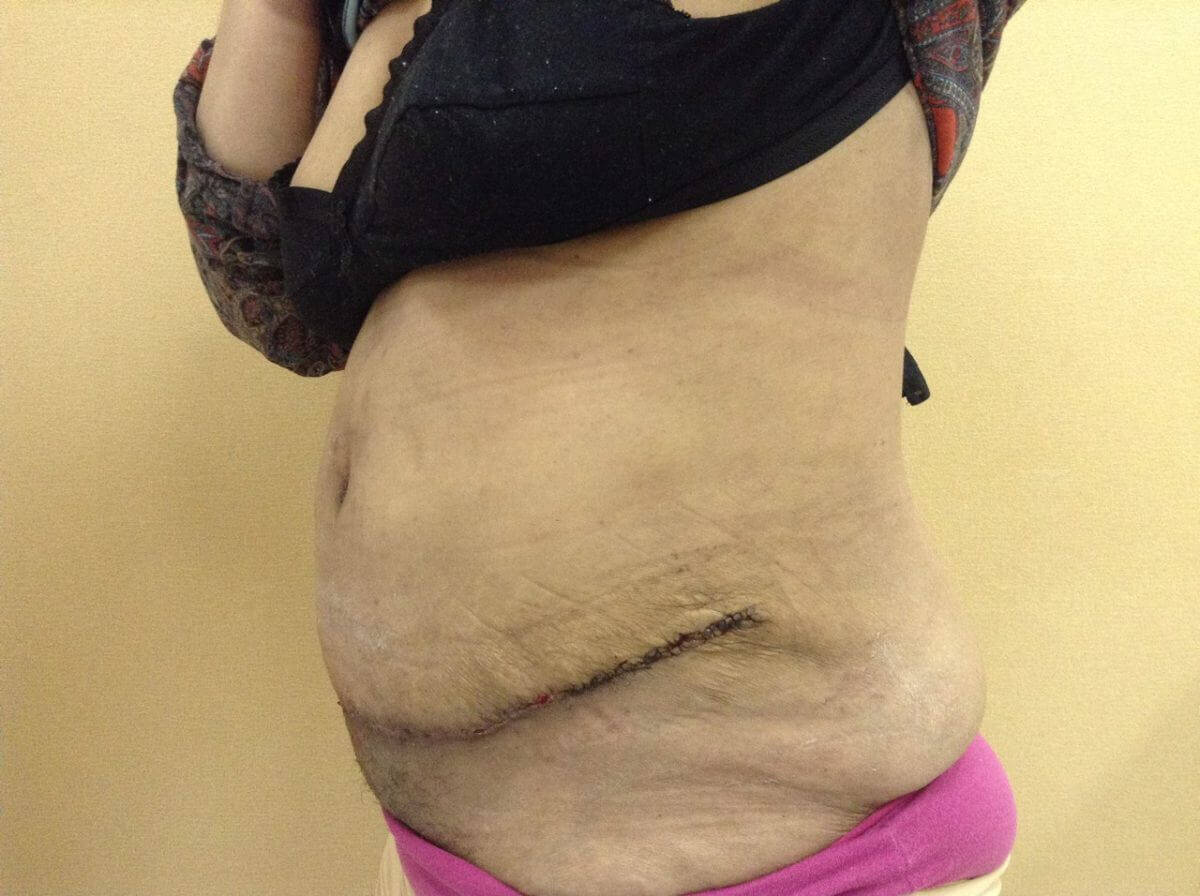
ABDOMINOPLASTY WITH UMBILICAL HERNIA REPAIR.
BEFORE
AFTER
In all aesthetic interventions on body and face permanent results depend on the patient’s stable weight ( +-5 kilos). That means we choose to operate on our patients when they have a “normal”, acceptable to them weight, which should remain relatively stable in the future.
RECONSTRUCTION OF CONGENITAL OR ACCUTE DIFORMITIES OR DEFFECTS